US research team uses Unitree G1 humanoid robot to perform surgery on live pigs, the world’s first
By and Tao Mingyang Published: Jul 12, 2026 04:02 PM

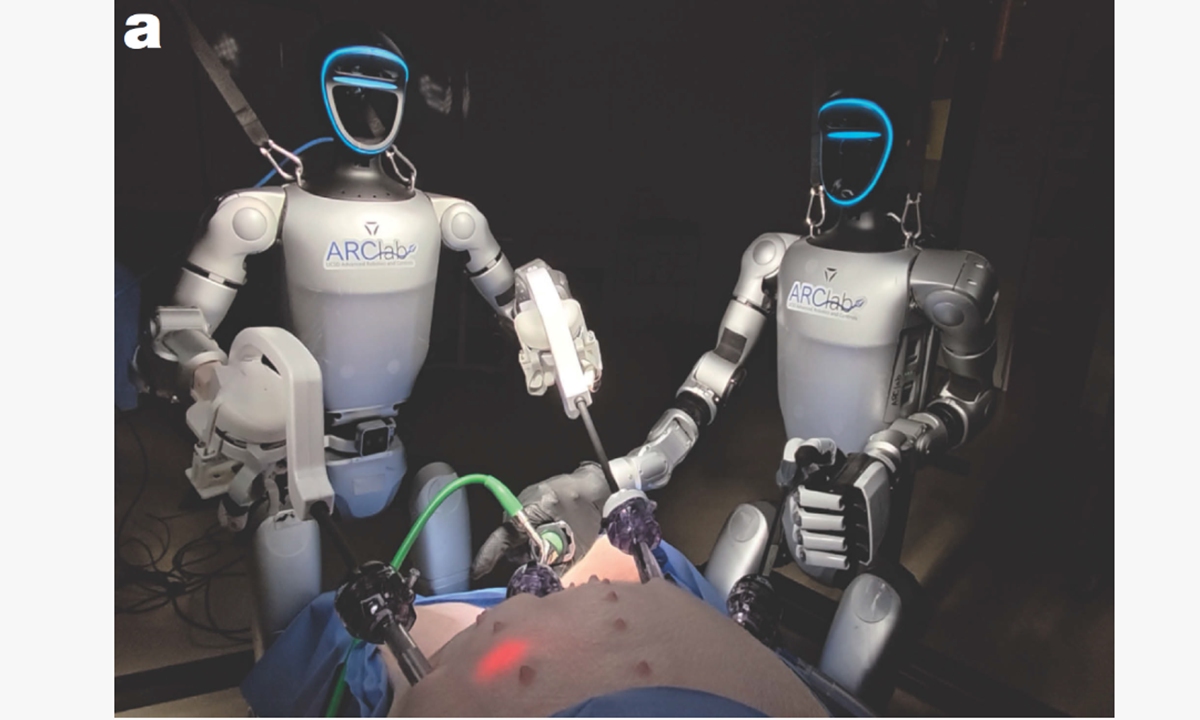
Unitree's G1 humanoid robots perform live porcine laparoscopic cholecystectomies. Photo: Screenshot of a study published in Nature
A US research team has used Unitree G1 humanoid robot to successfully perform standard laparoscopic cholecystectomies on two live pigs, during which the robot is teleoperated to manipulate manual laparoscopic instruments, according to a study published in Nature seen by the Global Times, marking the world's first use of a humanoid robot surgical system to perform a complete minimally invasive surgical workflow on live animals.
According to the article, the team developed a teleoperation framework that enables a humanoid robot to perform laparoscopic manipulation using manual wristed instruments. Unitree G1 humanoid was chosen because it is "an economical and commercially available system representative of contemporary general-purpose humanoids."
A Unitree spokesperson confirmed that the operating humanoid robot was Unitree's G1 series. He told the Global Times on Sunday that if the surgery is true, then "humanoid robot has at least achieved the precision required to perform surgery on pigs."
Chen Jing, vice president of the Technology and Strategy Research Institute, told the Global Times on Sunday that he believes that the pig surgery using a common humanoid robot is of landmark significance because "it verified a new path toward replacing specialized surgery platforms with general-purpose one."
"It means that there is no need to build a separate hardware ecosystem exclusively for medical robotic use, and humanoid robots can enter the operating room directly with proper adaptation," Chen said.
According to public information, the da Vinci system was originally priced between $1.5-2.5 million, with annual maintenance costing approximately $175,000. Meanwhile, according to an introduction on Unitree's official website, a baseline Unitree's G1 model has a starting price of 85,000 yuan and a weight of 35 kilograms.
He also highlighted Chinese-made robotics' overwhelming edges compared with others, including mature commercial platform which features dexterous hands and an open-source teleoperation framework, as well as strong support from a large research community. "They also excel in cost, size and general-purpose adaptation."
According to the study published on Nature, two surgeries on porcine models were performed by Unitree G1. The surgeries were performed followed a standard laparoscopic workflow, with one console surgeon and one bedside assistant. To ensure consistency, a single senior surgeon performed all procedures from the robotic console using the humanoid platform, whereas bedside assistance was provided by either another senior surgeon or a clinical fellow experienced in laparoscopic surgery. The assistant managed camera control, tissue retraction, exposure and bedside adjustments such as camera cleaning and instrument adjustments.
Also, during a brief interval in the first case, a second humanoid robot was used for camera holding and retraction. Both cases were completed robotically, with neither procedure required conversion to conventional laparoscopy or open surgery, demonstrating the initial feasibility of the humanoid robotic system for in vivo use. The first case was completed without major intraoperative complications. In the second case, minor biliary spillage and liver-bed bleeding occurred, which were managed with suction and electrocautery.
According to the study, in the O-ring replacement task, or a standardized ring transfer procedure, error rates for novices operating the humanoid robot were comparable to the da Vinci Research Kit (dVRK)- a standard surgical robotics research platform-and markedly lower than manual performance. For the more demanding fundamentals of laparoscopic surgery (FLS) peg-transfer task, the humanoid achieved intermediate results, surpassing manual operation in both speed and accuracy, though it lagged behind the more established dVRK system in these two indexes.
Researchers described the pig surgery as "establishing an early, quantitative benchmark for humanoid surgical performance in vivo." They also noted that surgeon feedback highlighted "a distinct gap between technical feasibility and clinical readiness," pointing out that constraints in range of motion, force generation, and the need for frequent recalibration significantly increased both cognitive and operational burden.
With regards to wider application, the article noted that "once clinically ready, humanoid platforms may help address several limitations inherent to contemporary robotic surgery… By providing a versatile humanoid platform at a lower cost, these systems may improve accessibility and broaden the availability of robotic-assisted surgical care."
Chen believed that if the method of "humanoid robotic surgery technology plus virtual programming" matures, the system could be rapidly deployed in remote regions or field hospitals. However, it may still take at least five to ten years for the technology to enter the surgery room, and for the short term, humanoid robots are more likely to function as teleoperated assistants for remote medical procedures or tasks like retraction and camera holding, rather than acting as independent lead surgeons, he noted.
Expert said that considering that dVRK has been developed over more than 20 years, humanoid robots will need substantial advancements in precision, latency, sterile design, and autonomous decision-making before they can truly enter routine clinical use in the operating room.
RELATED ARTICLES